Justice & Brain Injury
Brain Injury 101
What is a Brain Injury – Information with * Adapted with permission from Dr. Lemsky’s book
What is a Brain Injury?
An Acquired Brain Injury (ABI) is an injury that occurs any time after birth which disrupts the normal functioning of the brain.
There are two basic kinds of Acquired Brain Injuries: Traumatic and Non-Traumatic.
Traumatic brain injury (TBI) occurs when there is a more severe force that causes the brain to move in the skull, (such as a blow to the skull or sudden jerking of the head).
The signs of a brain injury include:
- Any period of loss of consciousness or decreased consciousness;
- Any loss of memory for events immediately before (retrograde) or after the injury (post-traumatic amnesia);
- Neurological deficits such as weakness, loss of balance and coordination, disruption of vision, or change in speech, language, or senses:
Confusion, disorientation, slowed thinking, or difficulty concentrating.
Non-traumatic brain injury occurs when the brain is damaged by disease (such as a tumour or infection), exposure to a toxic substance (such as drugs or solvents), loss of oxygen to the brain (such as a strangulation), or stroke (bleeding or a blood clot in the brain that causes damage to brain tissue).
Causes of Traumatic brain Injury
The most common causes of traumatic brain injury are: motor vehicle crashes, falls, being struck by an object or being a victim of a physical assault
Measuring the severity of traumatic brain
➔ Medical documents may reference the Glasgow Coma Scale (GCS). This scale is a measure of how much a person’s level of consciousness was altered by the injury.
➔ The GCS is an important element in rating the severity of TBI after injury.
➔ A GCS of 9 or less indicates a Severe Brain Injury
➔ 9-12 Indicates a Moderate Brain Injury
➔ 13 + indicates a Minor Brain Injury
What to expect after Brain Injury
➔ Recovery from a brain injury is unique to each person and is determined by a combination of the following:
– Medical history (general health)
– History of previous injury
– History of substance use / substance use disorder
– Nature of the injury itself (the type and location of the injury, the depth and duration of coma, complications after injury such as low blood pressure or loss of oxygen to the brain)
– Obvious areas of damage in the brain being visible on medical images
➔ The vast majority of people – roughly 70 to 85% – will recover fully within weeks to months after a mild brain injury.
➔ People with moderate injuries may have lasting problems, but are generally able to return to many aspects of their pre-injury life.
➔ People with severe brain injuries generally spend time in hospital and often have lasting effects that may impact most or even all aspects of their daily lives
➔ Once a person has had one brain injury they are at increased risk for additional brain injuries.
➔ The cumulative effect of the number of brain injuries that a person experiences throughout their life is important to understand.
Research has shown that experiencing two or more brain injuries that were severe enough to have caused loss of consciousness, even if they were mild, leads to a greater risk of experiencing lasting mental health and cognitive problems.
Brain injury Guidelines
For further information on brain injury guidelines and best practices for brain injury rehabilitation visit the Ontario Neurotrauma Foundation Brain Injury Guidelines.
Social Determinants of Health and Brain Injury
➔ While TBI occurs across all levels of sociodemographic status, evidence suggests a strong socio-economic gradient with individuals from disadvantaged backgrounds being at greater risk. (Colantonio et al., 2014; Hwang et al., 2008., Williams et. all., 2006)
➔ We also know that the sequelae of TBI are most often superimposed on pre-existing language and literacy impairments as well as mental health, substance use and addiction challenges. (Hughes et al., 2012; Snow et al., 2012., Snow et al., 2016).
➔ In a recent study of women in the sex trade, 95% had sustained head injuries at some point in their lives, either by being hit in the head with objects and/or having their heads slammed into objects. 61% said their injury had occurred as a result of their sex work.
➔ 92% of women living in domestic violence shelters reported their partners hit them in the head more than once (Sojourner Centre).
➔ There are over 20 million women in the U.S. who have an undiagnosed TBI.
➔ A Toronto Study from St Michael’s Hospital found that 58% of homeless men and 42% of homeless women in Toronto have a brain injury, and the average age of first brain injury was 17 years old. 87% of those injuries occurred before they became homeless.
➔ This population is at risk for experiencing seizures, mental health problems and poorer physical health.
➔ Another study from Michael’s Hospital found that living with brain injury and being homeless harms a person’s wellbeing, and as such this population is:
➔ 5 times more likely to have visited an emergency room in the past year
➔ Twice as likely to have been arrested in the previous year
➔ Three times as likely to have been victim of a physical assault in the past year
Prevalence of Brain Injury
➔ TBI is the number one cause of death and disability in Canadians under the age of 40.
➔ The annual global incidence of TBI is greater than that of Breast cancer, HIV/AIDS, Spinal Cord Injury and Multiple Sclerosis COMBINED. Yet TBI does not receive the public awareness and funding of these other conditions.
➔ Over 500,000 Canadian sustain a TBI each year and incidence rates are rising.
➔ A well known TBI statistic states that men have twice the rate of TBI as women. Having said that, given the high rate of women who have experienced Intimate Partner Violence who report they have been hit in the head, often more than once, it is very likely there are large numbers of women with undiagnosed TBI.
➔ Concussion is the third most common sports injury.
➔ 15 – 24 year-olds are the most at risk for TBI. Other risk groups by age are the very young (0 – 4 years old) and adults over the age of 75.
Introduction
This section will explore the intersection between brain injury and substance use. There is significant research to indicate an overlap of brain injury, substance use and criminal behaviour. These factors should be taken into account when assisting someone with a brain injury navigate the justice system.
Research in the area has found that:
- Children and young adults experiencing TBI are at greater risk of developing substance use disorders and engaging in criminal activities compared to those without TBI (1)
- In a study of substance abuse and crime patterns, 327 patients with various severities of TBI reported a high preinjury incidence of moderate and heavy drinking; 81% and 47% among those with and without arrest histories, respectively (2)
- There is an Increased risk for legal difficulties/ criminal misconduct with ongoing substance use following a TBI (3)
Information contained in the sections below have been adapted with permission from Dr. Lemsky’s book.
What is a substance use disorder?
➔ A substance use disorder is diagnosed when the repeated use of alcohol and / or drugs causes a significant problem with health and / or a failure to meet major responsibilities at work, school or home.
➔ Addiction is often defined as a complex, chronic disease that affects the functioning of both the brain and the body. When addicted, people continue to use a substance even though they know that it is causing them harm. It is described as a chronic, relapsing disorder because the changes in the brain circuits involved in processing rewards, stress and self-management can last a very long time—well after a person has stopped using drugs.
➔ Often the term addiction is used when a substance use disorder is severe. The term misuse may be used to describe excessive or risky use that has not developed into an addiction.
Symptoms of problematic substance use
- Using more of the substance that was intended, and for a longer period of time
- A desire to cut back and being unable to do so
- Spending a great deal of time getting, using or recovering from the use of the substance
- Strong cravings/desire to use the substance
- Use of the substance interferes with regular activities or obligations
- Use of the substance continues despite the fact that it causes significant problems
- Using when it is physically risky to use
- Using is causing physical or psychological problems (or making them worse)
- Using more of the substance to get the same effects (tolerance)
- Feeling symptoms of withdrawal, and using the substance to feel ‘normal’
Consider that:
- 82% of Canadians drink 7 or fewer drinks per week
- Only 6% of Canadians drink 15 or more drinks per week
The risks that come with drinking increase at the number of drinks rises
Substance use and brain injury – Facts
➔ 25 – 30% of people who are treated for brain injury were intoxicated at the time of the injury
➔ More than half of all people who are admitted to Acquired Brain Injury (ABI) rehabilitation programs have a history of substance use
➔ Brain injury early in life more than doubles the risk for problems with substance use later in life
➔ 20% of people will develop a new problem with substance use after brain injury
➔ Using substances increases the risk of re-injury
➔ People with brain injury and substance use disorders are also at high risk to have other mental health problems
Navigating the mental health and addictions system
- After a brain injury, it may be more difficult for someone to participate in treatment for substance use disorders because most treatment programs are based on the idea that a person has or can develop the ability to manage the urge to use. For a person with a brain injury self-management and self-control are often a problem
- Difficulties with memory may also make it more difficult for a person with brain injury to participate in treatment of substance use. People with brain injury may have a much harder time remembering appointments, conversations or decisions about treatments, including any actions they agree to take.
Treatment programs will often involve multiple supports and phases: individual treatment, enrollment in formal services, residential and/or out- patient, peer support, family. Since most services are voluntary so your family member, once accepted, can opt out themselves at any point in the treatment process
Resources
NIH: Understanding Druge Use and Addiction (US national healthcare service)
Canadian Centre on Substance Use and Addiction (CCSUA)
CAMH: Canada’s Lower-risk guidelines
Centre for Addiction and Mental Health (CAMH)
Government of Canada: Get Help with Substance Use
NIH: Drugs of Abuse (US national healthcare service)
Alcoholics Anonymous (AA)
National Institute on Alcohol Use and Alcoholism: Treatment for Alcohol Problems (US national healthcare service)
- Matheson, F.I., Mclsaac, K.E., Fung, K., Stewart, L.A., Wilton, G., Keown, L.A., Nathens, A.B., Colantonio, A., & Moineddin, R. (2020). Association between traumatic brain injury and prison charges: a population-based cohort study. Journal of Brain Injury, 1-8. DOI: 10.1080/02699052.2020.1753114
- https://www.houston.va.gov/docs/research/Graham.pdf
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6171742/
There are many physical, emotional, cognitive and behavioural challenges that can accompany a brain injury. The Ontario Brain Injury Association (OBIA) has created an in-depth resource that explains the different challenges that can affect someone with a brain injury and how to help manage them. Click here to visit their page.
What is a concurrent disorder?
A concurrent disorder is when symptoms of two or more disorders are present in the same person at the same time. In brain injury, the term concurrent disorder is used for situations where a person has a neurological disorder (brain injury) in addition to either a mental illness, substance use disorder or both.
Mental health disorders are a set of changes in thinking, feelings or behaviour that occur over a period of time and interfere with a person’s life. For example, a major depression occurs when a mood change has lasted a period of more than two weeks without relief, and has made it difficult for a person to engage in their normal life activities.
Neurological Disorders an acquired brain injury is considered a neurological disorder. Other brain diseases such as epilepsy, Parkinson’s disease or multiple sclerosis are also considered neurological disorders.
Research has shown that people who have had mental health issues may not recover as well from mild brain injuries.
How common are concurrent disorders?
➔ Studies have found that as many as 70% of all people served by programs specializing in concurrent mental health and addictions problems also have a history of brain injury with loss of consciousness.
➔ This is another reason why it is important to screen any legal clients for a potential brain injury and investigate the severity of their injury and how it applies to their case. *Link to screening tool
➔ The most common mental health problems to develop after brain injury are depression, anxiety and substance use disorders. While estimates vary greatly, there are studies that have found that more than half of all survivors of brain injury (including those with mild brain injuries) will experience significant symptoms of depression and/or anxious mood at some point in their recovery.
➔ Brain injury may increase the likelihood of having a mental health problem, but the reverse is also true. The risk of sustaining a brain injury seems to increase when a person is living with a mental health disorder or they are using substances in a problematic way. For example, it is easy to understand that people are more likely to injure themselves while intoxicated.
➔ We should not forget the importance of the psychological and social effects of living with brain injury related changes in thinking, behaviour and function. There may be uncomfortable changes like dizziness or vision changes and headache. There can be changes in thinking or physical abilities that have resulted in life changes and feelings of loss. There are plenty of reasons to worry about the future or feel sad about changes. Brain injury creates life stress, and that can result in changes in mental health.
The basics of self-regulation
➔ Emotions can be understood as the body’s way of sensing and communicating what is happening in the environment. The pleasant sensations of being happy send feedback to our brains that something good is happening. When we’re anxious, our body is telling us something dangerous is happening. When there’s a good match between how we’re feeling and what’s happening in the environment (accurate sensing) all goes well. But there are times when having too much emotion interferes with our ability to think clearly, and get things done. The reverse is also true, failing to respond to the environment with the right emotion (such as fear) might cause a person to take risks and get hurt, or failing to experience good feelings may lead to substance use or other compulsive behaviours.
➔ To function well we have to be able to manage our emotional state using feedback from the environment, but also make judgements about what our body is telling us to figure out the best way to respond.
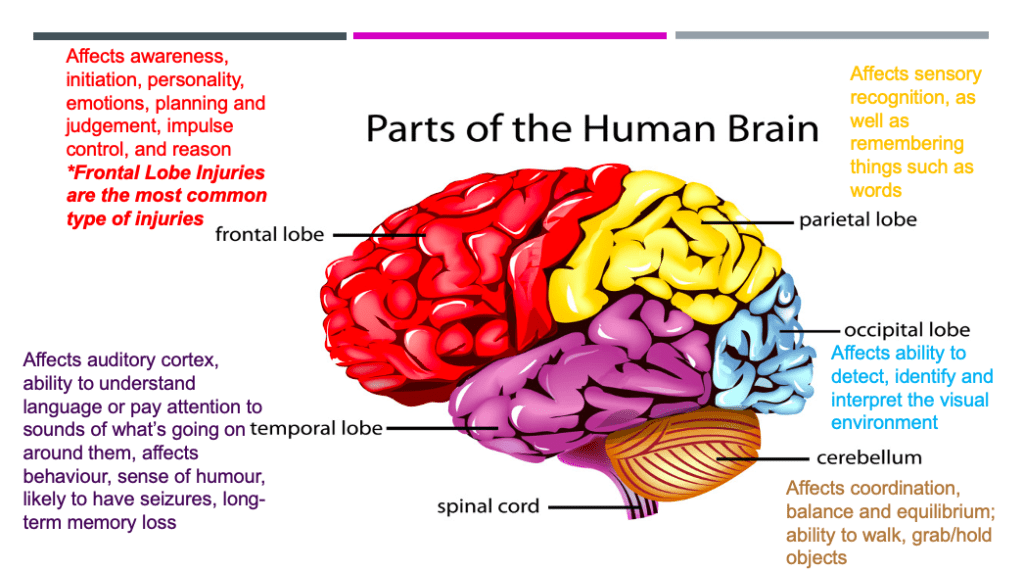
Brain changes that cause behavioural problems
➔ Problems with behaviour and mood occur when the emotional (limbic) system goes out of balance with the frontal lobes. When there is a problem with the functioning of the reasoning and planning centres in the brain, emotional responses may seem to carry more weight and people can appear depressed, anxious and have more trouble controlling their anger. They may also have trouble resisting temptations, or be more prone to developing addictions or obsessions. Similar problems may happen when the damage is done to the connections between different parts of the brain.
Post-Traumatic Stress Disorder
➔ Post-Traumatic Stress Disorder (PTSD) is common after mild to moderately severe brain injury. People who have limited memory loss at time of the injury are most likely to develop PTSD. But symptoms of PTSD, such as irritability, avoidance of sights and sounds or situations related to the traumatic situation, and being on edge or easily startled may be seen in people who have only a limited ability to recall the event that caused the injury. For example, it is pretty common for survivors of car accidents to be wary of busy streets or cars and to react strongly to traffic noises or sirens.
➔ When a brain injury is sustained during combat or in wartime, the likelihood of PTSD seems to be significantly higher. It could be that stress of wartime plays a role in a person’s recovery or that having a brain injury makes the difficulties in controlling emotions that occur with PTSD worse. People who have symptoms of PTSD may find it is more difficult to recover from brain injuries.
Psychotic Disorders
Psychotic disorders are much less common than mood disorders after brain injury. But brain injury and substance use may increase the likelihood of a person developing a psychotic disorder, particularly if the person has a genetic or family history of psychotic disorder
Mood disorders
➔ Just like the general population, depression and anxiety are the most common mental health problems to develop after brain injury of any severity.
➔ It is estimated that half of all adults living with moderate to severe brain injury experience depression and/or anxiety that is severe enough to impact their quality of life and ability to do the activities of daily living.
➔ Anxiety and depression are observed in more than half of all brain injury survivors.
➔ Most researchers and clinicians agree that both direct changes to the brain and the need to cope with a lot of changes after brain injury can cause depressed or anxious mood.
Bi-Polar disorder
We all have ups and downs in mood, but when a person has bi-polar disorder the swings in mood are much greater. In typical bi-polar disorder, a person experiences both periods of depressed mood and periods of mania. Mania is when a person’s mood seems unusually high, they seem to be overconfident, have ideas about being very powerful and may have an excess of physical energy to start but not be able to finish projects. They have trouble sleeping and may act without thinking in a way that is different from their normal personality. Usually each of these different types of moods last for a period of weeks or even months. But sometimes a person’s mood can flip back and forth suddenly and often between depression and mania. There is no specific pattern to periods of depression or mania which can happen regularly or very infrequently.
Resources
Centre for Addiction and Mental Health (CAMH)
The Centre for Addiction and Mental Health (CAMH) is Canada’s largest mental health and addiction teaching hospital, as well as one of the world’s leading research centres in the area of addiction and mental health. CAMH combines clinical care, research, education, policy development and health promotion to help transform the lives of people affected by mental health and addiction issues.
For specific health information through CAMH, visit their Health Information Page.
More Mental Health Resources
Canadian Mental Health Association – Understanding Mental Illness
Mental Health Commission of Canada
National Alliance on Mental Health (NAMI)
Crisis Lines
Canada Suicide Prevention Service
Crisis phone: 1-833-456-4566;
Text: 45645
Email: info@CrisisServicesCanada.ca
Website: http://www.crisisservicescanada.ca
Telephone counselling and support for anyone thinking about or affected by suicide.
Toronto Distress Centre
Crisis Line: (416) 408-4357
Website: http://www.torontodistresscentre.com
Telephone counselling and support for anyone thinking about or affected by suicide.
Toronto Seniors Helpline
Telephone: 416-217-2077 OR 1-877-621-2077
Website: https://torontoseniorshelpline.ca
Face-to-face crisis assessments and crisis support to seniors in Toronto who are 65+. Clients are triaged, phone support offered whenever possible.
Online Support
The Big White Wall
Website: https://www.bigwhitewall.com/?lang=en-ca
Online peer support community for mental health including anxiety, depression and other common mental health issues. Peer to peer, anonymous conversation moderated 24 hours a day, seven days a week by trained practitioners.
Telephone & Online Support
Bounceback
Telephone: 1-866-345-0224
Website: https://bouncebackontario.ca/
Free ongoing Cognitive Behavioural Therapy (CBT) program that provides guided mental health support for adults and youth, which utilizes workbooks, online videos, and phone coaching. Must register.
ConnexOntario
Telephone: 1-866-531-2600
Website: https://www.connexontario.ca
Information and referral on addiction and mental health services in Ontario.
Telephone Support – Adults 25 +
Yonge Street Mission – Virtual Walk In Counselling
Telephone: 416 355-3568
Monday to Friday from 10 am to 4:30 pm Thursdays 10 am – 7:30 pm
Telephone counselling to those feeling anxious or distressed.
Telephone Support – Youth
Kids Help Phone
Telephone: 1-800-668-6868
Website: https://kidshelpphone.ca/
Canadian nationwide 24/7 mental health support service which includes professional counselling, information and referral, and volunteer-led text-based support to youth (18 and under) in English and French.
Good2Talk
Telephone: 1-866-925-5454
Website: https://good2talk.ca/
A texting and phone call service that provides confidential support to post-secondary students
Yonge Street Mission – Virtual Walk In Counselling (Ages 16-24)
Telephone: 416 929-9614 ext 2269
Monday to Thursday from 10 am to 4:30 pm
Telephone counselling to those feeling anxious or distressed.